Part 1:
| |
We will use this module to look at the histopathology of the common skin cancers, particularly in situations where the histology directs the treatment modality or margins of excision. By understanding how tumours grow you can better conceive of why one treatment is better than another.
Other examples of histopathology will be found in the Resources section and links will be found from this module to the relevant parts.
Basal Cell Carcinomas To all intents and purposes BCCs do not metastasise but an infitrating or recurrent bcc is a different kettle of fish from a well circumscribed small nodular bcc. Once you see the histology of these lesions you will understand why! The nodular BCC has sharp edges meaning that clearance by 1-2 mm is fine whereas the infiltrating edges of a infiltrating or morphoeic bcc need 5-7 mm clearance clinically to be 90% certain of removing all the tumour. Have a look at the three cases below.
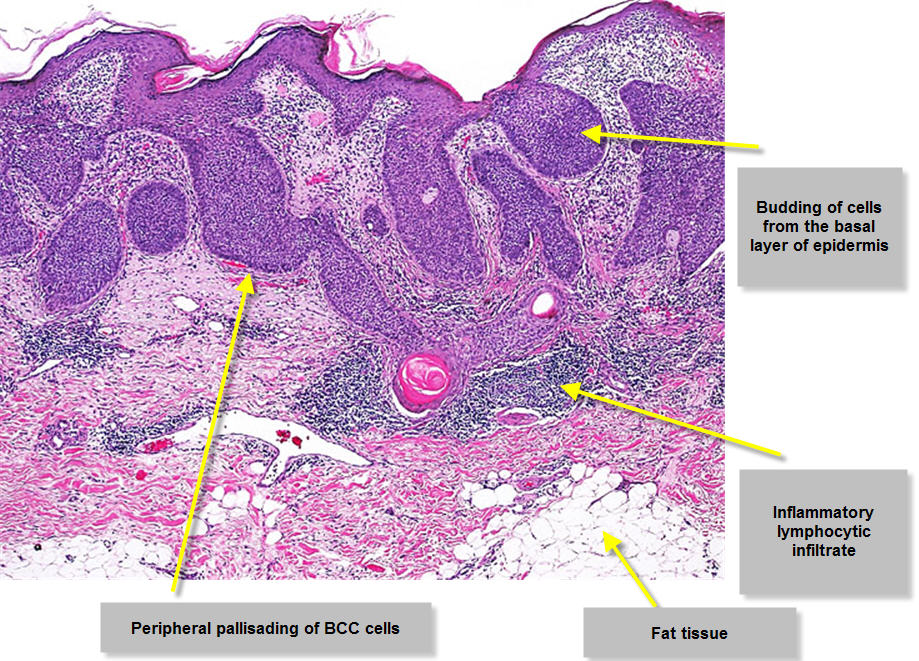
Image 1 Superficial Multifocal BCC
The superficial multifocal BCC buds off the epidermis. You can see the bluish tumour cells arising from different points of the epidermis with relatively normal epidermis inbetween. Some of these buds may also arise from the edge of a hair follicle. If you look at the outer edge of a bud you will see the cells are arranged in a regular columnar fashion like bricks lined up on the basement membrane. This is known as pallisading and is a characteristic feature of BCCs. This slide also shows some inflammation underlying the tumour. Because of this histology a superficial bcc is often reported as fully excised when the excision site has simply passed between two of these buds through normal appearing epidermis. Many of these buds at the outer edge of a superficial multifocal bcc are so small that they are not visible clinically.
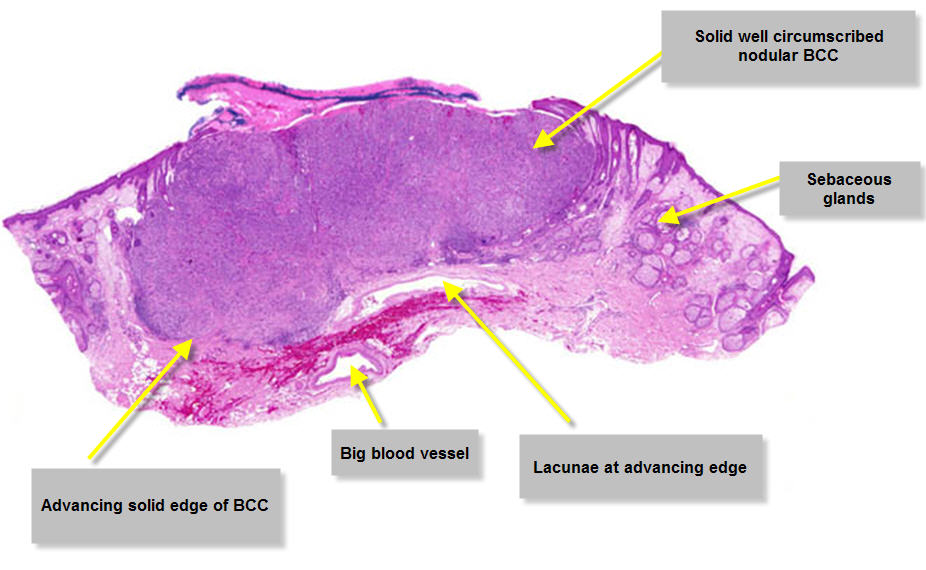
Image 2 Nodular BCC
A nodular BCC obviously has a different look to a superficial multifocal BCC. It is a solid mass of cells advancing as a solid edge. There may still be some peripheral pallisading of cells at the advancing edge. There may also be some separation of the BCC from the tissues it is advancing into. These are called lacunae or tumour spaces.
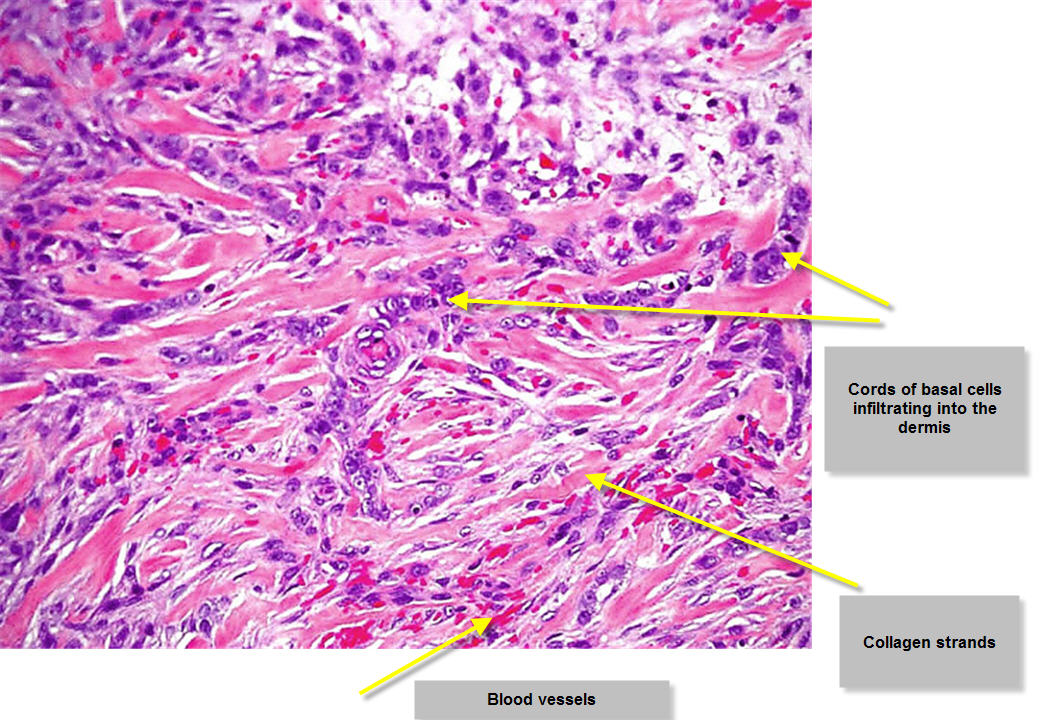
Image 3 Infiltrating BCC
The infiltrating BCC does not have a solid advancing edge but instead has cords of cells which infiltrate into the surrounding tissues between the collagen bundles. These cords may be quite thin ie only one or two cells thick. They can be far in advance of the presumed clinical tumour edge. This explains why these tumours are often inadequately excised because the apparent tumour edge does not correlate well with the histologically defined edge. Now view these other examples of the histopathology of BCCs
You may find this site useful if you want more information on dermatopathology See Dermatopathology Made Simple
| |
   |
Part 2:
| |
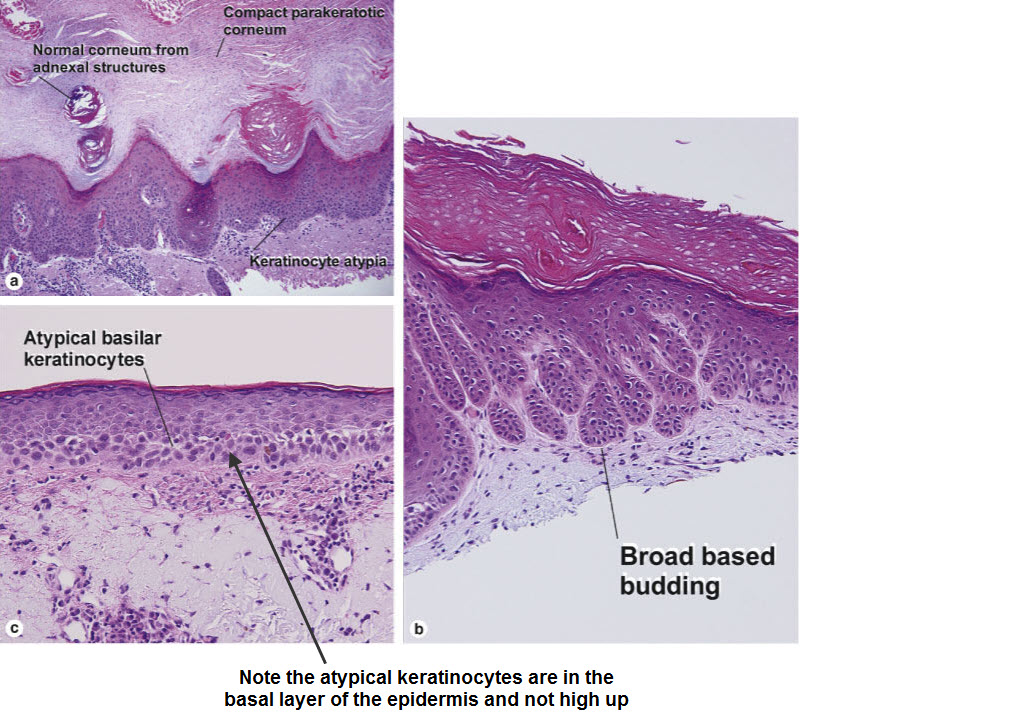
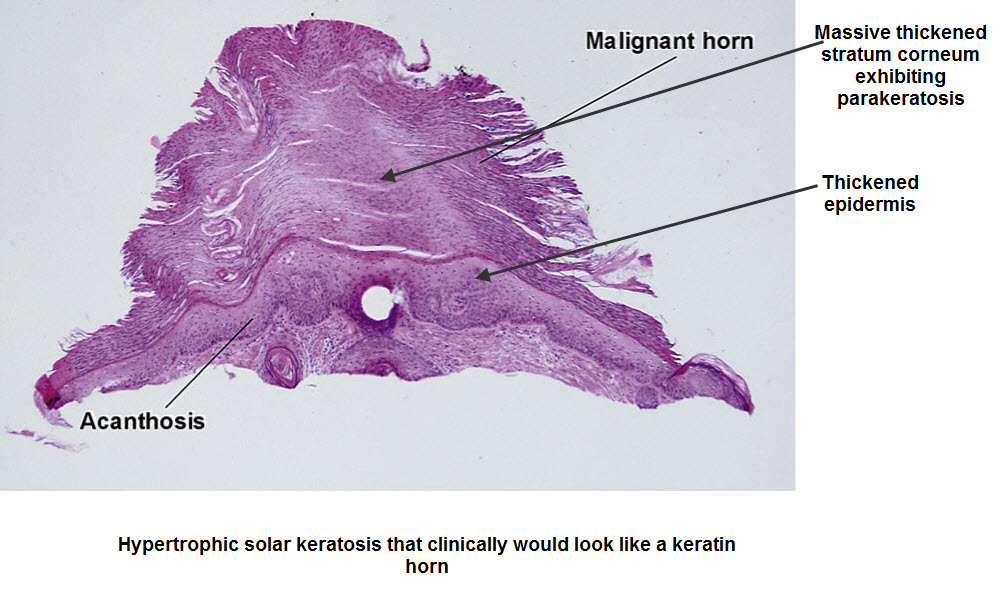
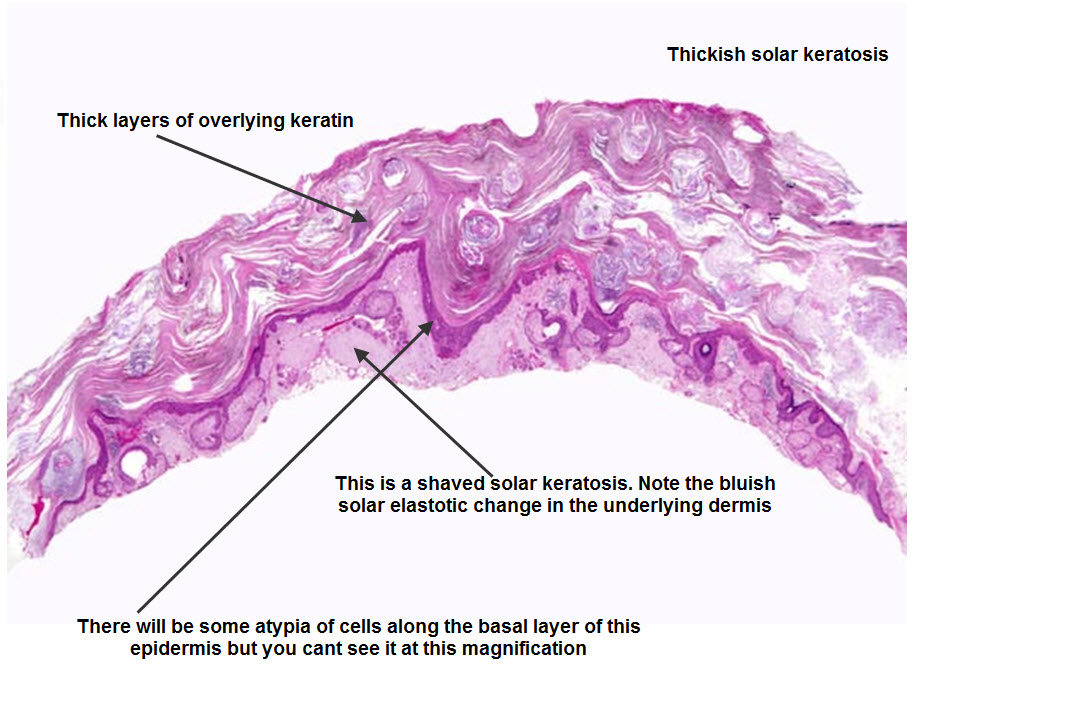
Solar keratoses are really early SCCs with the initial atypia confined to the basal layer of cells of the epidermis. Now most people falsely think that the atypia should be of the upper layer of cells in the epidermis because the sun involves these cells most but remember that keratinocytes originate from basal layer cells and migrate up. The UV damages these basal cells and the damage starts deep. There is also abnormal keratinization from these cells reflected in the thick hard keratin scale on the surface of a solar keratosis.
Clinical correlation You can see that keratolytics will only soften and remove the thickened overlying layer of keratin but do nothing for the atypical layers of cells. Also this thick layer of keratin prevents the penetration of Metvix ( aminolaevulinic acid ) cream in photodynamic therapy (PDT). | |
   |
Part 3:
| |
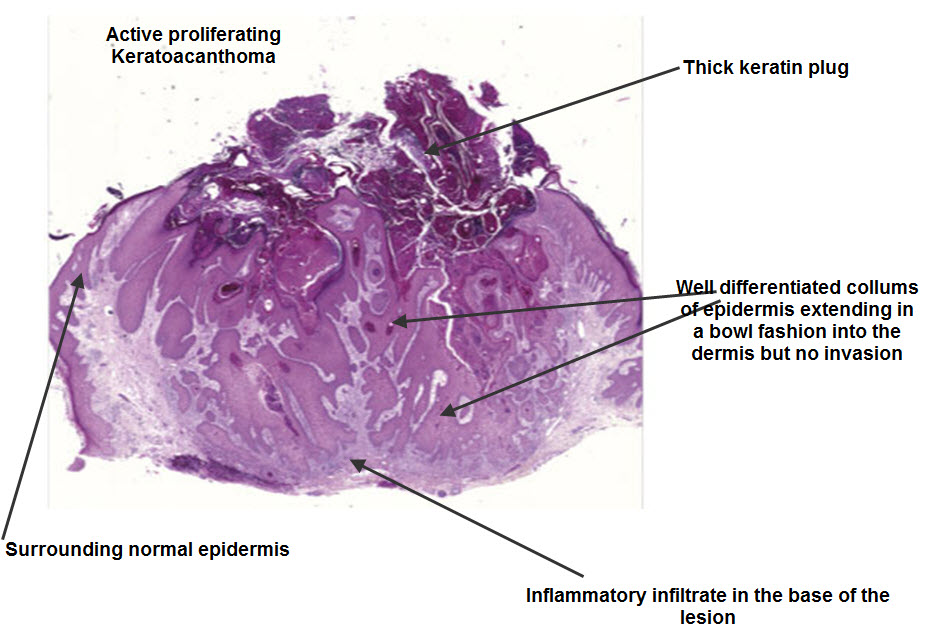
Keratoacanthomas are rapidly growing "benign" variants of SCC in that they do not metastasise. They have pale coloured glassy cells and a pushing lower edge rather than an infiltrating edge. Nonetheless they are often reported as well differentiated SCCs.
Clinical correlation Many dermatologists simply curette these lesions rather than formally excise them.Because of their pushing edge they usually just shell out. The important thing is to remove them quickly because they can double in size in a two week period. Some can involute on their own but doi not bet on it!
| |
 |
Part 4:
| |
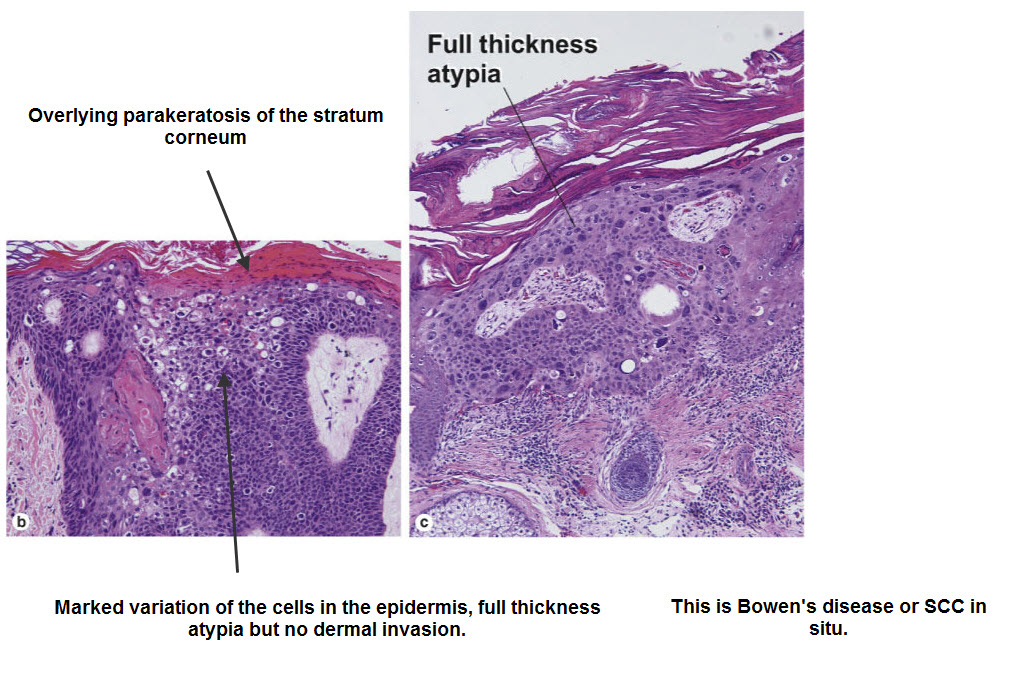
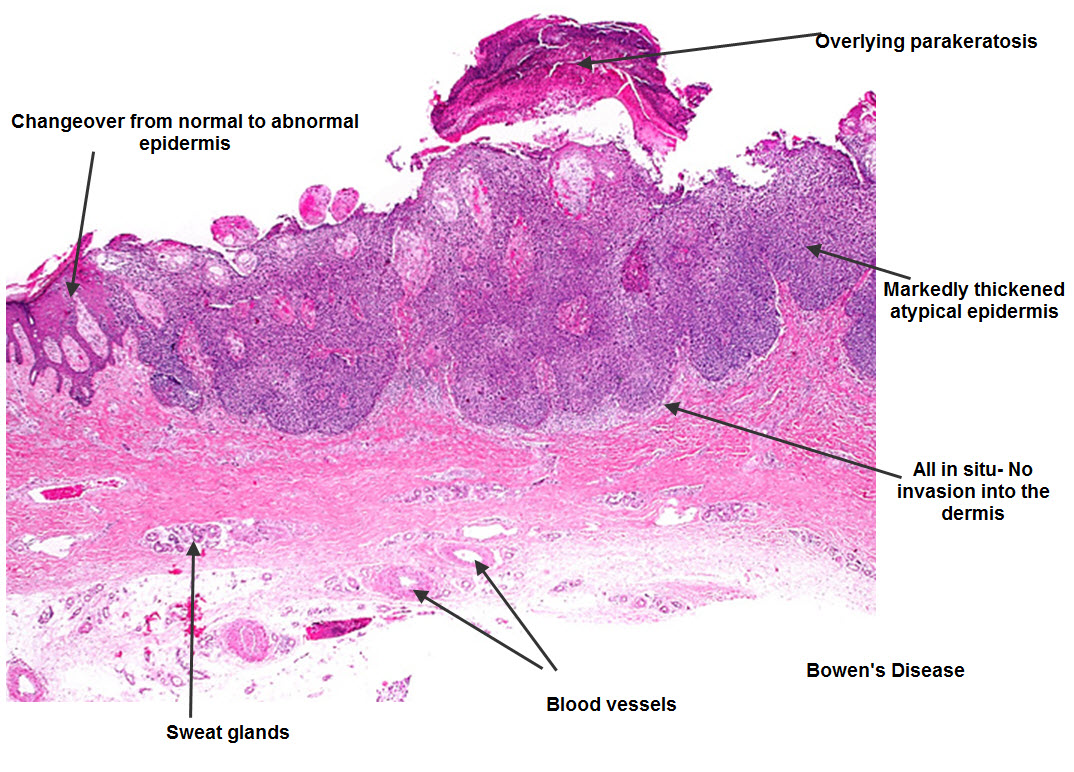
SCC in situ or Bowen's disease.
The keratinocyte atypia extends throughout the whole epidermis from the basal layer to the stratum corneum but is confined by the basement membrane under the basal cells and does not penetrate through into the dermis. Sometimes you see mitoses in some of the keratinocytes. If Bowens disease is secondary to an oncogenic virus then you may see koilocytes high up in the epidermis representing viral involvement. This is common in Bowenoid papulosis on the genitals. Sometimes you will receive a report mentioning an area of Bowen's disease within a seborrhoeic keratosis but this may just be the benign clonal variant of a seb k! Conversely you might get a report of a clonal seb k when in fact it is Bowens disease. This is where your dermatoscope can be very useful. Clinical correlation Because the abnormal cells are confined to the epidermis these lesions can be treated by topical measures including Efudix, Aldara and PDT therapy but note that the wall of the hair follicle is an extention of the epidermis and Bowens disease will extend deeper from the surface in hair bearing areas. Sometimes PDT will not extend deeply enough and recurrences can happen as initial pinpoint lesions ascending up the follicle and spreading into the pale treated epidermis. This can also occur with the other topical modalities including cryotherapy but is least seen with Aldara. | |
  |
Part 5:
| |
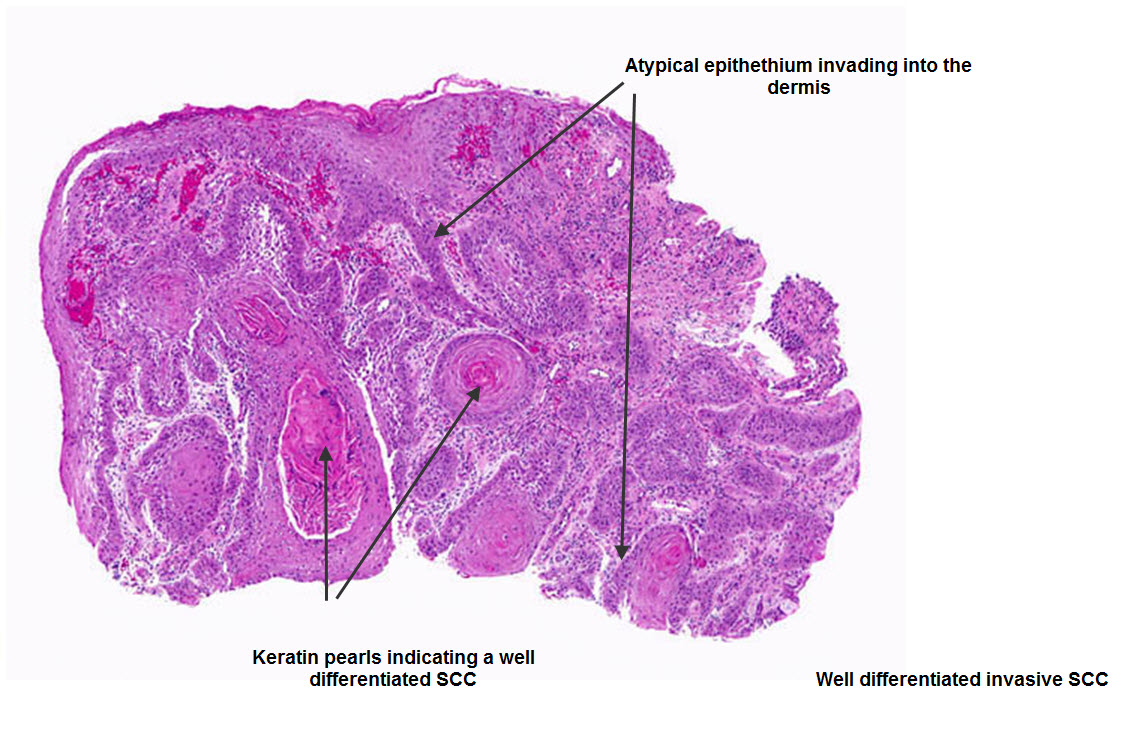
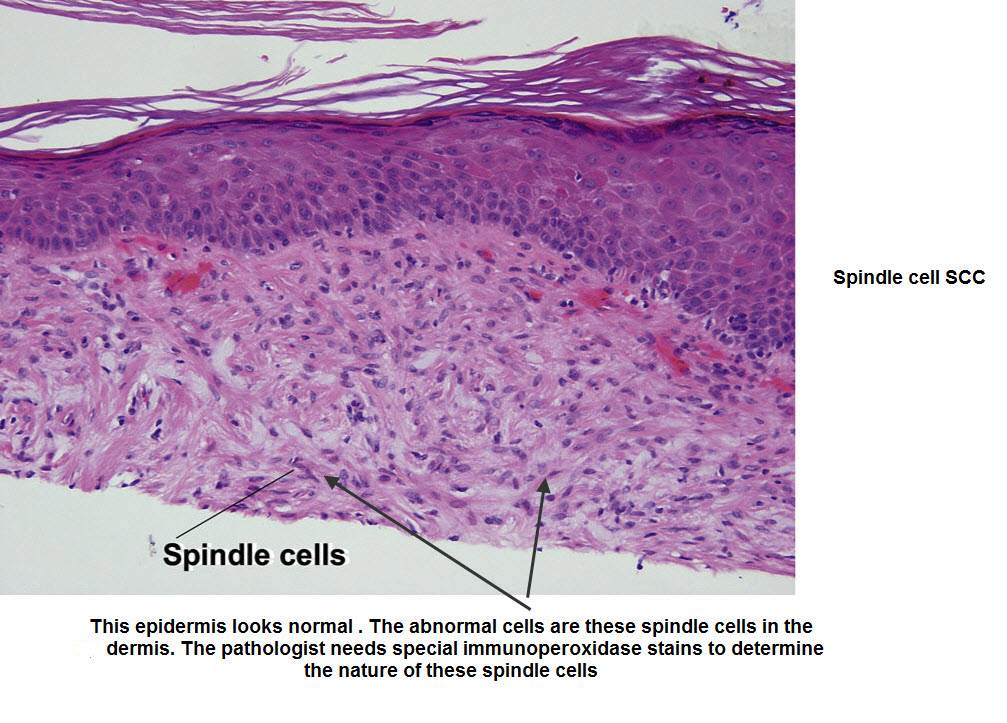
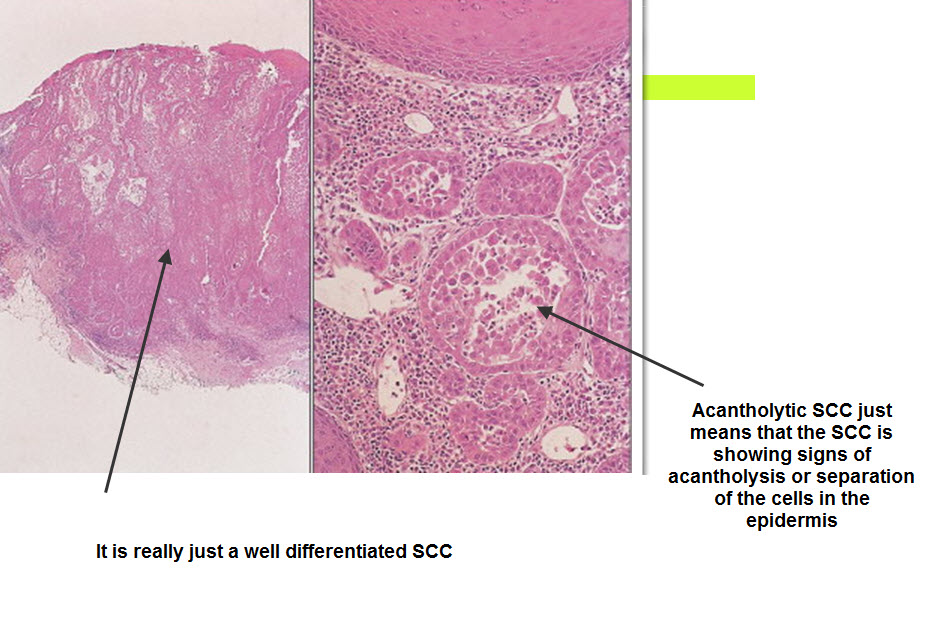
Invasive Squamous cell carcinoma These lesions are characterised by epidermal hyperplasia and a thickened sratum corneum. The tumour originates from the keratinocytes in the epidermis but invades through the basement membrane into the dermis. It may do it as frond like masses of cells with a pushing edge but also sometimes as spindle cells infitrating between the collagen bundles.
Clinical correlation An invasive SCC has a more firm base than an SCC in situ. Invasive SCCs are also reported as either well differentiated, moderately differentiated or poorly differentiated. The latter are particularly likely to spread both locally via the lymphatics and around nerves. They require excision margins of 5 mm if possible. Margins of 1-2 mms for excised poorly differentiated SCCs should be regarded as inadequately excised and should be re excised to prevent local recurrence.
Have a look at this video by Dr McColl with Virtual slide technology which looks at actual slides of these conditions. When it runs press pause and the reset the 360 to 720 and click the little box at the side with the arrows pointing out. This will make it display in HD full screen. Press ESC on your computer to revert to the reduced playing size.
| |
   |
Part 6:
| |
The video below lasts about 25 mins. It is a video presentation of a post by Cliff Rosendahl in the SCCANZ Dermoscopy Blog in which he looked at both the dermatoscopy and Histology of benign nevi. Concentrate on the distribution of the nevus cells either on the sides of the rete ridges or also filling the dermal papillae and how this changes the dermatoscopic appearance.
This video lasts 9 mins and looks at a case in the SCCANZ blog with clinical and histological images.
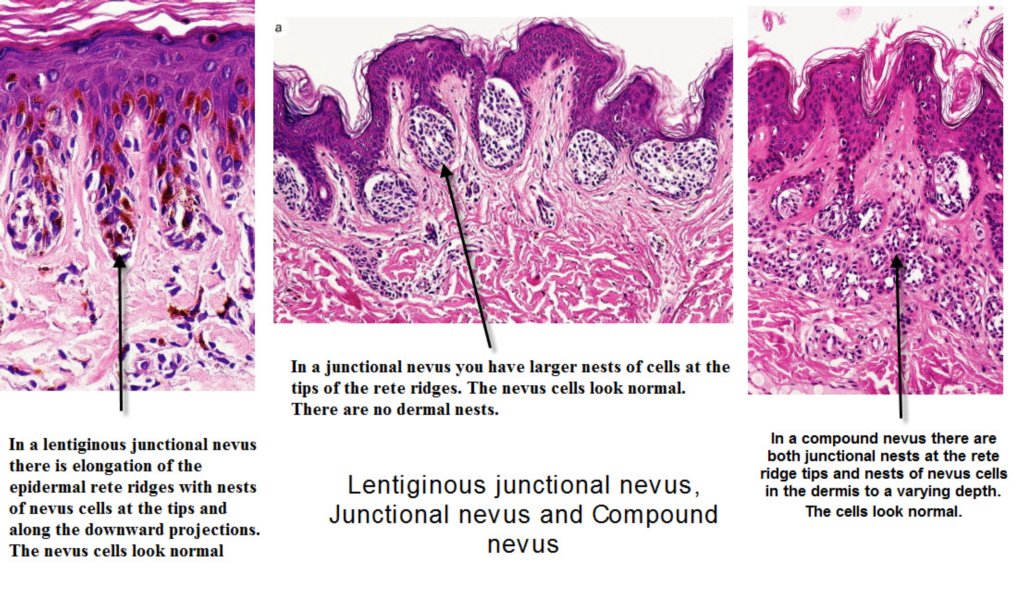
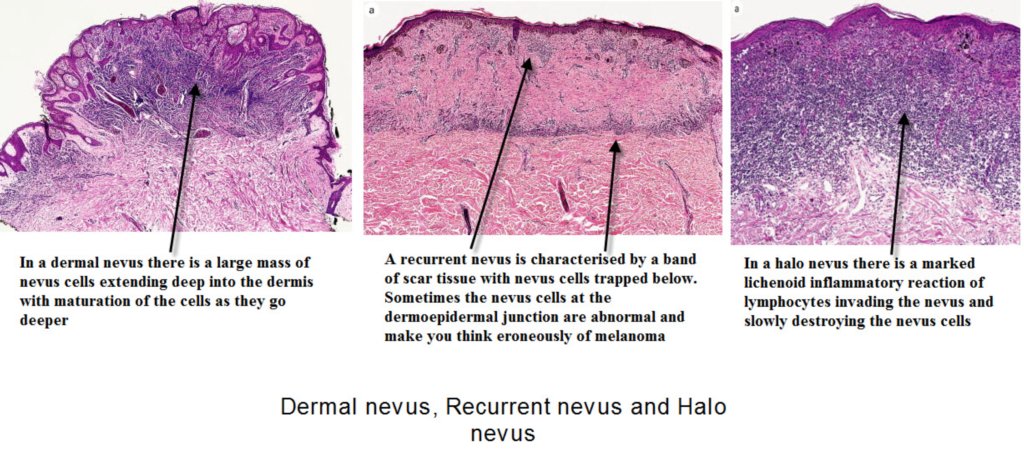
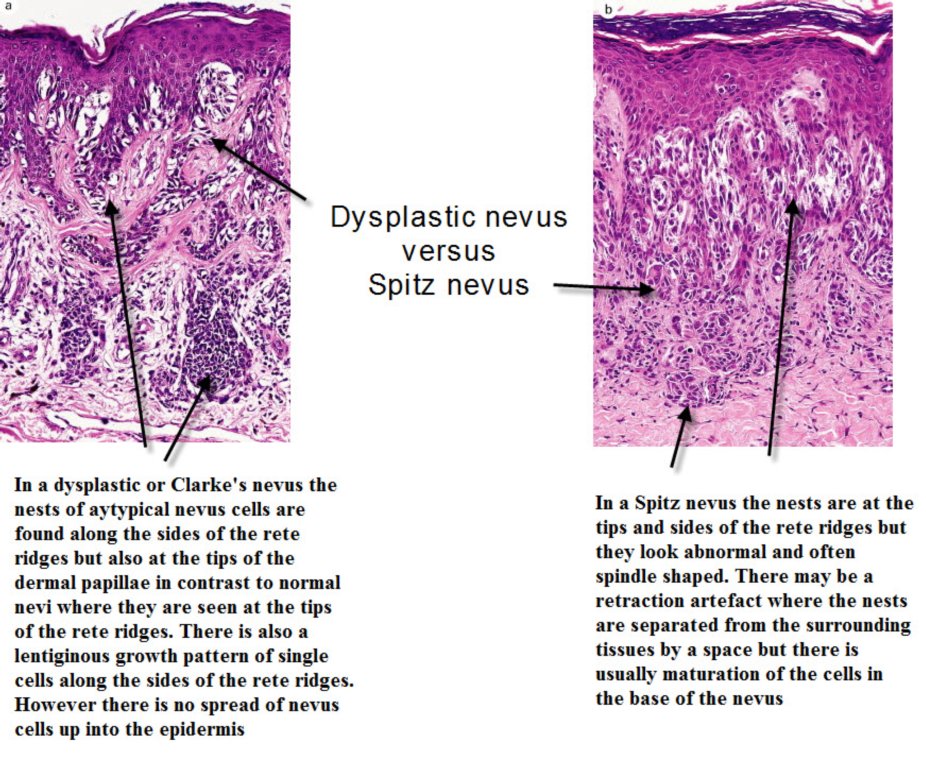
Benign nevi Histologically benign nevi do not show chaos. They have nests of normal looking nevus cells or melanocytes, without mitoses or abnormal nuclei, and show maturation of cells as you go deeper. They are usually well circumscribed lesions. There is a rare variant of melanoma called a nevoid melanoma, seen in younger people, presenting as a rapidly growing dark lesion, which can be misdiagnosed as a benign nevus. It is the commonest reason for pathologists to be sued for missing the diagnosis of melanoma. A Spitz nevus is a benign nevus which disobeys the rules for benign nevi but has some other characteristic features I have outlined in the image below. Dysplastic nevi are clinically atypical nevi varying from normal in size, colour and shape, which show histological features which overlap with those of melanoma especially if classed as severely dysplastic. Clinical correlation The clinical importance of this is that if you excise a pigmented lesion with narrow 1-2 mm margins and it is reported as severely dysplastic, you should re excise to 5mm margins effectively managing it as a melanoma in situ. Have a look at this Jeff Keir SCCANZ Blog Presentation on Close to the Border Line regarding severely dysplastic nevi and melanoma. | |
   |
Part 7:
| |
This video is an overview of the histopathology of pigmented skin lesions.
Viewing this content requires Silverlight. You can download Silverlight from http://www.silverlight.net/getstarted/silverlight3.
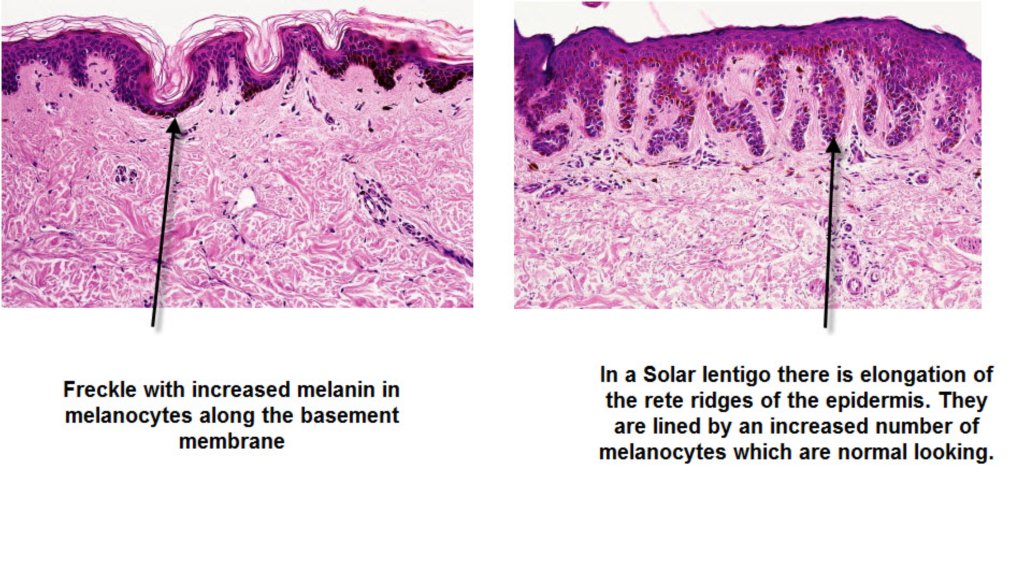
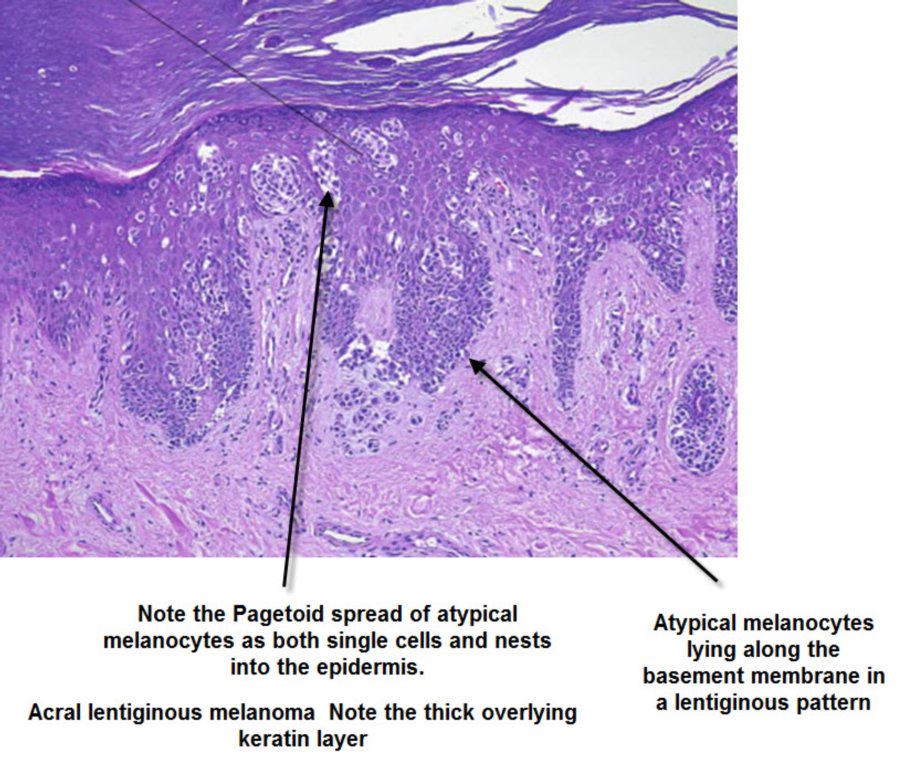
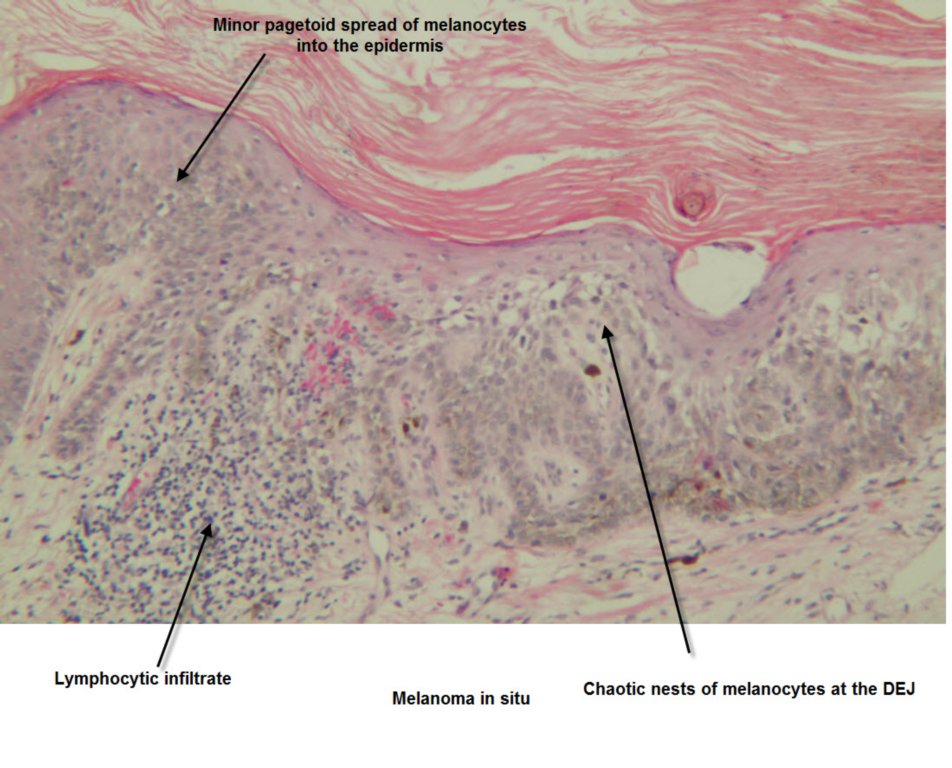
Solar lentigo, Lentigo maligna, Melanoma in situ I am not meaning that these lesions represent a progression to melanoma but clinically it can be difficult to decide between these diagnoses especially for larger pigmented lesions on the face. Have a look at the first clinical image below and note the progression of colour and thickness from the lower cheek to the lower eyelid areas. A biopsy taken from each area would show a different histology with an increasing level of chaos. ( The latter concept was first mentioned to me by Cliff Rosendahl who initially applied it to dermatoscopy images.) A solar lentigo is a benign lesion made up of increased numbers of benign melanocytes producing increased amounts of melanin and arranged without nesting along the basement membrane. A Lentigo maligna is an abnormal increase in number, size and shape of melanocytes arranged along the basement membrane in single file or a lentiginous pattern with a little bit of nesting accepted. Often the process extends down hair follicles. Some people also call this lentiginous melanoma or just plain melanoma in situ. | |
  |
Part 8:
| |
Invasive Melanoma Here nests of atypical melanocytes invade both into the dermis and up into the epidermis. The phenomenon of spread of atypical melanocytes up into the upper layers of the epidermis is known as Pagetoid spread and is a feature of superficial spreading melanomas.
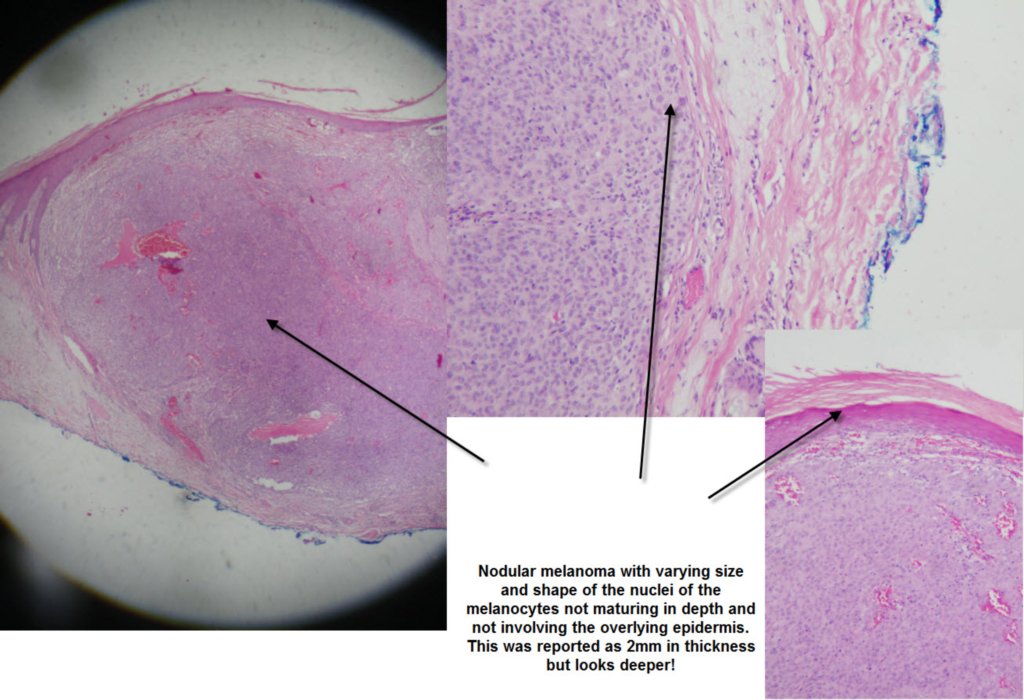
Nodular melanomas have little or no epidermal involvement and have a deep dermal component where the cells do not mature as you go deeper. They may also show mitoses and have a brisk lymphocytic infiltrate underneath them indicating an immune attack on the abnormal melanocytes. Desmoplastic melanoma is usually seen on the back with an overlying lentigo maligna like picture and underneath this are spindle celled melanocytes extending deeply into the dermis. They usually feel firm. Beware of shave biopsying these and only getting the upper lentigo maligna like part and hence misdiagnosing the thickness and worse prognosis of these lesions.
The following video looks at a presentation in the SCCANZ Blog by Cliff Rosendahl on the histology of Melanoma.
| |
   |
Part 9:
| |
Merkel cell carcinoma, Atypical fibroxanthoma,Extramammary Pagets disease
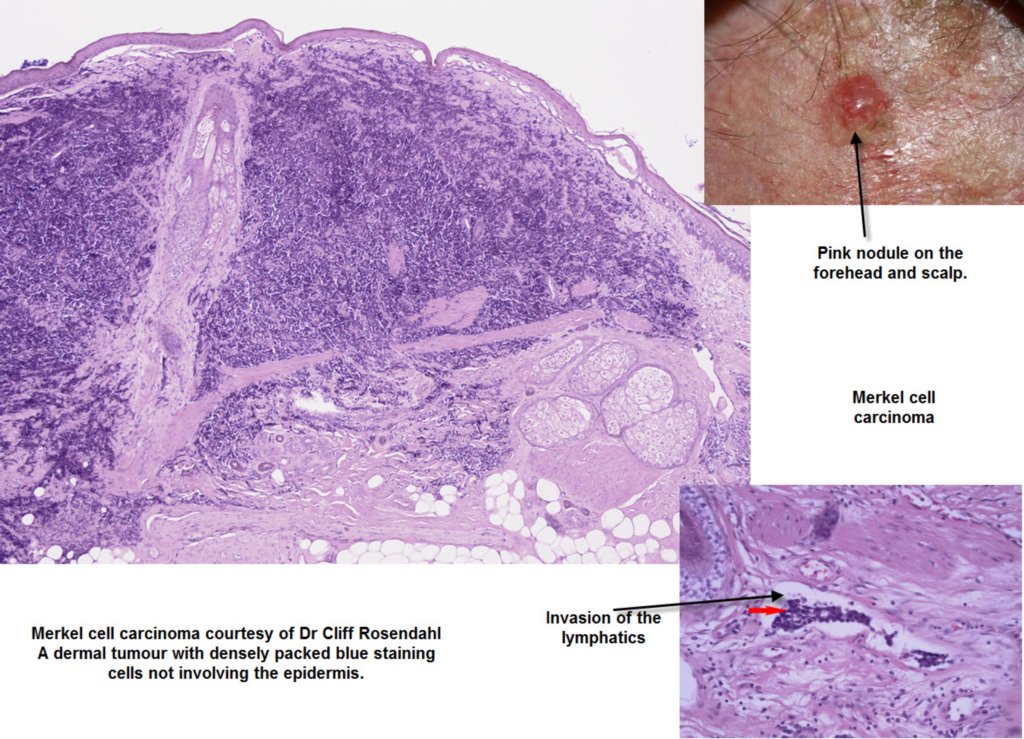
Merkel Cell Carcinoma is a small blue stained cell tumour which does not look too bad histologically but clinically has a worse prognosis than a thick melanoma. It is difficult to diagnose clinically even with a dermatoscope but should be considered in the differential diagnosis of any pink rapidly growing nodule.
View this excellent presentation from Cliff Rosendahl in the SCCANZ blog and check out the image link below on the case.
Atypical Fibroxanthoma is another differential of any pink rapidly growing nodule.It is often ulcerated and found on the ear. The histology shows bizarre atypical and sometimes multinucleated giant cells in the dermis with many spindle cells. Treat it like a poorly differentiated SC and excise with 5 mm margins. | |
 |
Part 10:
| |
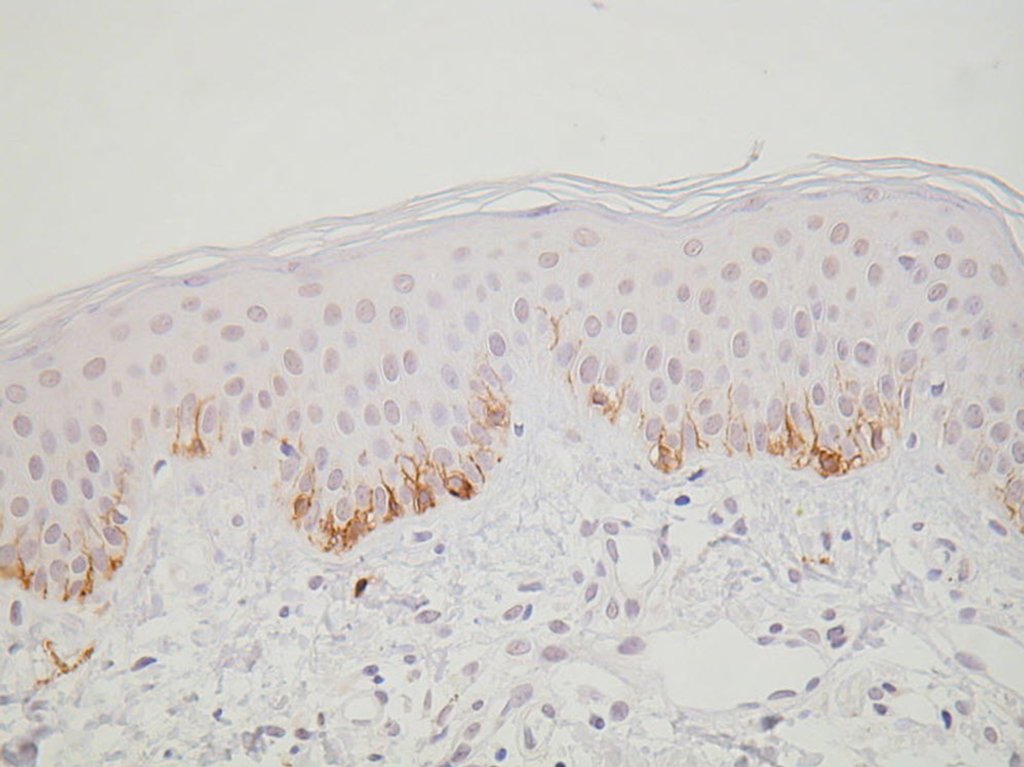
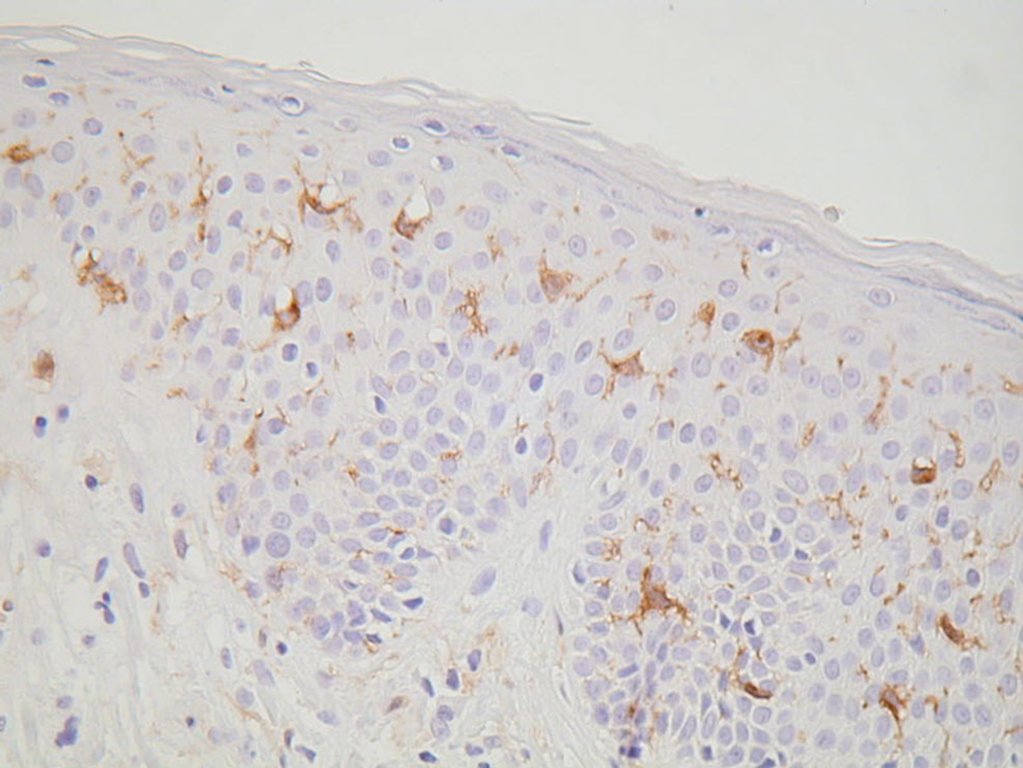
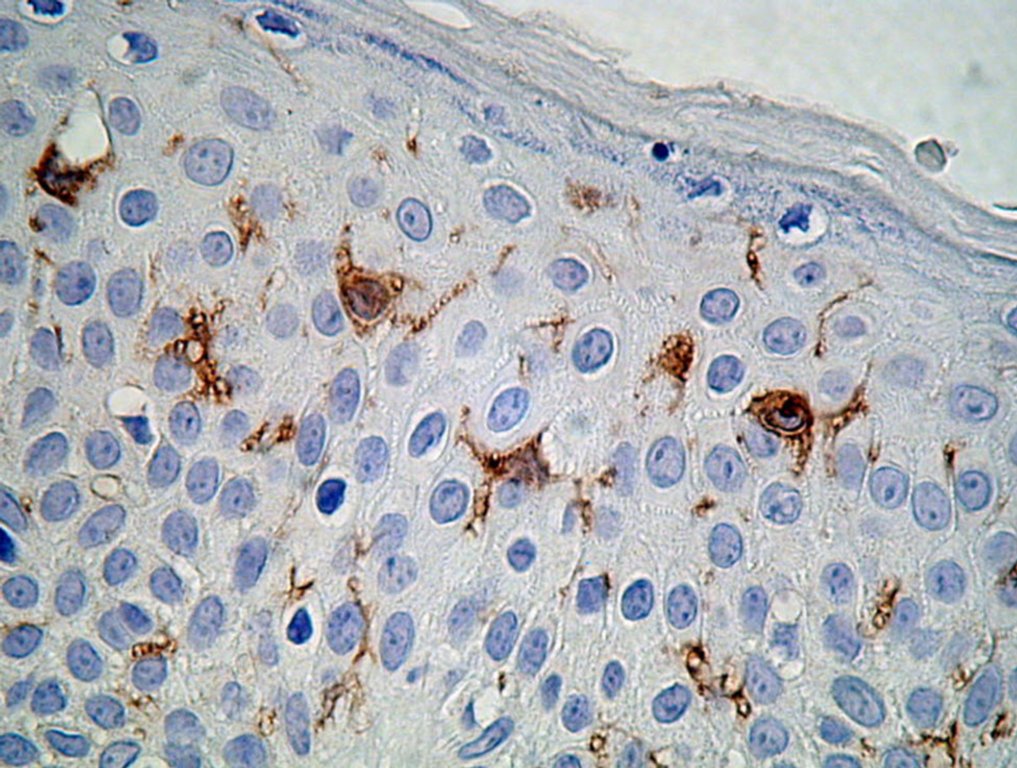
Special Stains in Histology Some people call these the brown stains or immune stains looking for specific antigens seen in particular tumours. They are useful for determining the cell of origin of say a spindle celled tumour which might be an poorly differentiated SCC or a Melanoma. They are also used in separating Extramammary Pagets disease and Bowens disease in the vulval area and confirming the identity of unusual vascular tumours such as Kaposis sarcoma and angiosarcoma. They can be done on the formaldeyde specimen you sent in initially.
If you want to play with a Virtual Microscope then Try this Virtual Microscope. Click on the button to view a slide in the Virtual Microscope. Concentrate on the skin tumours in this site.Use the + and - function in the little box on the top right side to enlarge the images and left click and hold to move around the image.
These two videos go through some of the images of skin tumours in these sites.
Part 1
Part 2
Modern Genetics in Skin Cancer Diagnosis. View this reference
| |
   |
No comments:
Post a Comment