Part 1:
|
Radiation Therapy
The key points of radiation therapy are that more than 90% of primary basal and squamous cell skin cancers can be cured by radiotherapy, so this is an excellent treatment modality, especially in the elderly. The problem with radiotherapy is that the scar gets worse with time so it tends to be reserved for people 60 years of age and above. Nonetheless the scar can be improved by what is known as fractionating therapy. This involves dividing the total dose into 20 or more treatments and delivering them over a 4-5 week period of time. Melanoma is poorly sensitive to radiotherapy but up to 25% can be treated. Lentigo maligna is probably best suited. Kaposi’s sarcoma is very radiosensitive and virtually all cases can be treated. Mycosis fungoides can also be treated as can B cell lymphoma of the skin. The latter will melt away with radiotherapy. The two types of radiation used are superficial x-radiation and electron beam radiation. Superficial quality x-rays are relatively low energy and will penetrate possibly 2cm beneath the skin. However an x-ray beam will lose about 10% of its energy after travelling only half a centimetre into the skin. It will drop to 50% of its maximum intensity at 2cm.
Electron beam radiation produces electrons which because they can be produced at different energy levels, can be made to travel set distances into the skin, probably to a maximum of about 3cm. Hence the intensity required to treat a superficial tumour can be very accurately measured. One has to be careful about the use of x-ray therapy near the eyes because of the danger of the induction of cataracts. Only a very small dose of x-rays is required to induce a cataract. Xray therapy also causes permanent hair loss.
Cosmetic Outcome
The cosmetic outcome of radiotherapy is directly related to the fractionation of the dose. The more the dose is fractionated the better the ultimate cosmetic outcome and the longer the duration of that cosmetic outcome. Radiotherapy compared to surgery is particularly good on those tumours involving the nose, the lip area and the ear and certainly should be considered for tumours of these areas in the elderly.
Field Therapy Radiotherapy is also very useful in treating a severely sun damaged bald scalp. It can get rid of multiple solar keratoses and SCC in situ and return the scalp to a smoothe state.
|
|
|
Part 2:
|
Basal and squamous cell skin cancers are usually treated with superficial x-ray therapy but the dose is fractionated to be more selective in removing tumour cells while preserving more radio resistant normal cells. Often treatments are fractionated over 20 to 25 doses to improve the ultimate cosmetic outcome. When tumours are treated in this way the five years recurrence rate for basal or squamous cell skin cancer is about 8%. Lesions that arise on areas of the skin that may be subject to trauma are not ideal for radiotherapy. Hence lesions on the hands and feet are best treated surgically.
Malignant Melanoma
Radiotherapy for malignant melanoma is mainly used in palliative therapy where surprisingly metastatic lesions do respond. In treating melanoma higher doses per fraction have to be given. However a trial was carried out in which a low dose, namely 250cGy (centi Grays) daily with 20 fractions was compared with 850 cGy weekly for four weeks and the response rates were around 25% for both.
Lentigo maligna and lentigo maligna melanoma have both been treated with radiotherapy. When a lentigo maligna was treated in the same fashion as a basal cell skin cancer, the lentigo maligna showed a good response with more than 85% regression. Radiotherapy is an appropriate therapy for lentigo maligna and lentigo maligna melanoma especially when it covers a large field area in an elderly patient.
In studies that have been done with other melanomas, prophylactic irradiation of high risk melanomas and the regional lymph glands improved the local regional control. However there was no overall improvement in survival. It has also been thought that the treatment of desmoplastic melanomas would be enhanced by giving radiotherapy to the excised area bed because of the propensity for this tumour to show infiltrative growth and perineural spread.
Kaposi’s sarcoma in all areas responds very well to conventional doses of radiotherapy. Similarly, localised areas of mycosis fungoides, a T cell lymphoma of the skin, will also respond to radiotherapy. A small proportion of patients though will suffer local recurrences. The technique used for treating mycosis fungoides depends really on the thickness of the lesion.
|
|
|
Part 3:
|
Cryosurgery
Key Points
If tissues are frozen below a certain temperature the cells will die. Melanocytes in the skin die at -15°c. Keratinocytes need a temperature of -50°c. This temperature has to be maintained for at least 15 seconds for these changes to occur. Cryotherapy properly carried out remains a viable treatment for non-melanomatous skin cancer. Its success though is very technique dependent and for it to be successful an adequate temperature has to be reached at the base of the tumour for the appropriate length of time.
Question
Who first used cryotherapy?
Answer
A Dr James Arnott in 1855 used a brine solution and achieved temperatures of
-24°c when he was treating certain cancerous tumours.
Question
What is the physiology of cryotherapy?
Answer
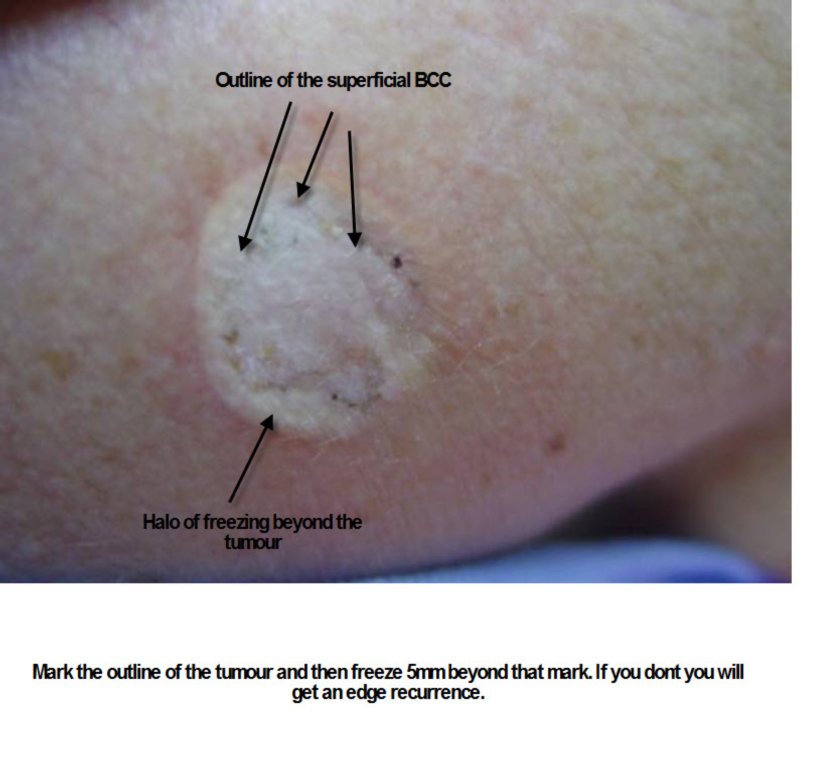
Essentially it is to freeze very quickly and allow it to thaw out very slowly and to do this several times. This rapid cooling produces intracellular ice crystals whereas slow freezing produces extracellular ice crystals. With intracellular crystals you are much more likely to get cell death. The cryogen that is used in most cryotherapy is liquid nitrogen though initially it was carbon dioxide snow. To assess the depth of freezing thermocouples are used. They are placed below the lesion and freezing occurs until the temperature reaches between -40°c and -60°c. If thermocouples are not used then the lateral extent of freezing and the duration of the thaw are the main assessment parameters used. Lesions are frozen from the centre outwards. The lateral progression of this halo freezing correlates to the depth. Larger superficial tumours such as basal cell skin cancers are frozen in a different manner because of their size and structure. They are sprayed over the surface to obtain depth of freezing with a halo of 1mm to 2mm whereas a nodular lesion is frozen from the centre and the halo is allowed to progress out beyond the tumour edge indicating an adequate depth will have been reached. Halo thaw time is another means of assessing adequate freezing. It should be between 60 and 90 seconds. If it is under 30 seconds the freeze is inadequate.
Question
What other aspects of the technique are important?
Answer
Adequate protection of surrounding structures. For example if near the eyes then wooden tongue depressors should be used to protect them. Rubber cones can be used to keep the spray within a certain area and pressure on these cones by reducing blood outflow can localise the freezing.
Question
How would you treat a thick skin tumour with liquid nitrogen?
Answer
Initially you would either curette or shave excise the lesion to decrease the thickness and then you would use a double freeze thaw spray on cryosurgery technique probably using neoprene cones. The de-bulking of the tumours decreases the depth of freezing you have to achieve.
Question
What sort of postoperative care do you use after cryotherapy?
Answer
Initially there is a lot of oozing and weeping so an absorbent dressing is necessary for a few days. Thereafter the area is washed with soap and water. An eschar forms and peels off. The time of peeling depends on the body site and the extent of the freezing, but it can be anywhere between three and six weeks.
|
|
|
Part 4:
|
Question
What are the cure rates of cryosurgery?
Answer
With carefully selected lesions the rates can be above 95% but this is where thick lesions have been curetted first and then frozen or shaved and frozen. It is obviously important to select your tumour and avoid areas where deep penetration of tumours is known to occur such as embryonic planes in the face and folds behind the ear.
Sometimes this technique is useful in the elderly where the whole treatment can be performed in one sitting. It is helpful if they are at a nursing home where dressings can be done but not essential. The primary advantages of cryotherapy are its relative low cost and surprising good cosmetic results coupled with a relatively high cure rate. It’s a technique that is especially useful for any infected sites. Provided you can get the tumour depth down to 4mm to 5mm then cryosurgery is very useful. Hence if you are going to tackle large tumours you should de-bulk them as much as possible first of all. Tumours that overlie cartilage are particularly useful to treat with cryotherapy because cartilage is tolerant of freezing. Also with other tumours with well defined margins even on the nose, cryotherapy can be quite useful and around the eye where the lacrimal duct will be preserved even if frozen to -70°c. Patients who have anticoagulation are not at increased risk of bleeding after cryosurgery.
Question
What tumours should you avoid with cryosurgery?
Answer
Major contraindications are aggressive tumours or tumours in areas where the tumour goes deep and recurrence is therefore likely. Tumours with indefinite margins should not be frozen and patients who have cold intolerant diseases such as Raynaud’s or cryoglobulinemia should have surgery rather than cryotherapy.
Question
What are the major side effects and complications?
Answer
After cryosurgery the first thing that happens is there is marked oedema and swelling. Less commonly is haemorrhage. Rarely in the elderly with thin tissue, nitrogen gas may penetrate under the skin and cause crepitus. Adequate post- operative analgesia is important in cryotherapy and sometimes the area being frozen can in fact be treated with local anaesthetic first. A migraine like headache may follow treatment of lesions on the temple or forehead. Cryosurgical syncope is probably a vasovagal response but it is not uncommon. Patients should therefore be treated sitting down. In patients who have diabetes it is always important to be careful about freezing lesions on the lower leg. Healing may be delayed, infection may occur and haemorrhage can occur.
Question
What are the long term reactions of cryotherapy?
Answer
Hypopigmentation and alopecia are two common long term reactions that cause the patient a lot of concern. Nerve damage can also occur. Melanocytes will be destroyed at -15°c for more than 10 seconds, so hypopigmentation is very common after the treatment of non-melanomatous skin cancer where the base of the lesion has to reach -60°c. The nerve dysfunction occurring after cryotherapy is rarely permanent. Sensation is depressed temporarily and usually returns after several months. If that nerve is near an area that is to be frozen, local anaesthetic can be injected between the tumour and the nerve. This is called ballooning. Hair follicles will be permanently disabled by 15 to 20 seconds of freezing. Hypertrophic scarring can also occur following cryotherapy but keloid scarring is much less likely than after surgery.
|
|
|
Part 5:
|
Laser Surgery for Skin Cancers
Key Points:
The main laser used is the carbon dioxide laser. It should only be considered for superficial basal and squamous cell skin cancers in non-hair bearing areas where formal surgical therapies are contra indicated. Patients who have carbon dioxide laser treatment of skin cancer should be followed up for recurrence, which might be expected in at least 20% of cases.
Question
What is the prime condition that can be treated with a carbon dioxide laser in the skin cancer field?
Answer
Actinic cheilitis. Actinic cheilitis or solar damage particularly to the lower lip can be treated very simply with a CO2 laser using a defocused mode. This gives very controlled superficial layer damage to the lip epithelium, which can be wiped away. Focal areas can be retreated. Healing takes place over a three week period and the lesion should be healed in a moist fashion with the application of antibiotic and other ointments such as Petrolatum. Areas of leukoplakia on the lower lip can be treated similarly once they have been biopsied to exclude any invasive squamous cell skin cancer. The latter is not suitable for laser therapy. SCC in situ particularly when it occurs on the glans penis or on other mucosal surfaces can be well treated with a carbon dioxide laser. Bowenoid papulosis of the genitalia can also be treated.
Basal cell skin cancers are more difficult. This is because variation in the histology can occur in up to 36% of cases with an infiltrative component being present and this would not be suitable for a CO2 laser. However patients with multiple basal cell carcinomas such as someone with the basal cell nevus syndrome may be successfully treated with a CO2 laser. The use of a CO2 laser can be combined with Curettage to give better results. Generally BCCs have to be lasered to the mid dermis level to get rid of them.
The CO2 laser has also been used in a lentigo maligna. Again the problem is that lentigo maligna often goes down sebaceous and hair follicles and CO2 laser treatment will not reach here. Nonetheless it is a modality that can be considered for an elderly individual who for one reason or another can not undergo surgery.
|
|
|
Part 6:
|
Oral Retinoids Oral retinoids such as NeoTigason (Acitretin) are particularly useful in reducing the rate of appeareance of SCCs in immunosupressed patients, particularly those after organ transplantation. More transplant patients die from skin cancer than failure of their transplanted organs. If you are developing more than 5 SCCs a year then the drug is indicated. Prescribing oral retinoids in Australia is restricted to Dermatologists and some Physicians because they are teratogenic in females. They cause marked dryness of mucosal surfaces and increased sun sensitivity. Usually you start with a dose of 10 mgs a day and gradually increase it to 25 mgs a day depending on side effects. The occassional patient can tolerate 50 mgs a day. You check FBC, LFTs , U/Es and triglyceride levels. High Triglycerides are a contraindication to prescribing these drugs because the retinoids will raise them further risking pancreatitis. You should not stop these drugs without slowly tailing them off as there is a rebound effect with the sudden eruption of multiple SCCs.
Topical Retinoids
Tretinoin topically can help treat actinic keratoses.
Adapalene (Differin) and Tazarotene (Zorax) topically are also partially effective at reducing solar keratoses.
Renal transplant patients treated with tretinoin (Retin A or Retrieve) developed fewer SCCs than those partients treated with placebo creams.
|
|
|
Part 7:
|
Alternative Topical therapies
1. Black salve (bloodroot, zinc chloride)Se previous Module.
2. Non steroidal anti inflamatories.
Aspirin orally has been shown to reduce SCC developement in severely sun damaged patients. However the effect is relatively weak. Another study published in the Archives of Dermatology in 2010 failed to show any benefit from several anti inflammatories including aspirin See Archives of Dermatology
Topical NSAIDs such as Diclofenac (Solareze) have a mild slow removal action on solar keratoses but the product has to be used daily for 16 weeks. The occassional patient can develope a severe allergic reaction to the topical. I rarely recommend it.
3. Skin cancer Vaccines.
Vaccines have been hoped to be the saviour of metastatic melanoma patients but up to date they have been singularly unsuccessful. Part of the problem is the fact that melanomas change when they metastasise and the tissue used in the vaccine which is usually derived from the original tumour does not antigenically represent the metastasis.
|
|
|
Part 8:
|
BRAF inhibitor drugs
Abstract
More than 80% of melanoma patients with an activating mutation in BRAF responded to treatment with PLX4032.
Introduction
Ever since researchers first described the role of BRAF mutations in melanoma, we have eagerly awaited a clinically effective anti-BRAF drug. A recent multicenter trial of a new agent seems to be the first step toward personalized medicine for melanoma. Investigators conducted a dose-escalation trial, with an extension phase, of PLX4032, an orally available kinase inhibitor of mutated BRAF; the co-developers of this agent supported the research. Fifty-five patients (49 with melanoma) were enrolled in an initial dose-escalation phase; another 32 patients with metastatic melanoma and tumors harboring the BRAF V600E mutation were enrolled in an extension phase.
In the first phase, the investigators analyzed antitumor activity and dose-limiting toxicity to arrive at a dose of 960 mg twice daily for the extension phase. Cutaneous squamous cell carcinomas (SCCs) occurred in 8 (15%) and 10 (31%) of the patients in the dose-escalation and extension cohorts, respectively, (median onset, 8 weeks). All but one of the SCCs were or had features of keratoacanthoma, and none required therapy discontinuation. Sixteen patients in the first phase harbored the BRAF V600E mutation; 11 (69%) had a response, 10 partial and 1 complete. Patients without BRAF mutations showed no evidence of tumor regression; four had progressive disease within the first 2 months of treatment. The extension phase included only patients with the BRAF V600E mutation. Of these 32 patients, 26 (81%) had a response, 2 complete and 24 partial. The estimated median progression-free survival among these patients at the time of analysis was more than 7 months.
Comment An unfortunate side effect of using these drugs is an increased developement of aggressive SCCs!.
|
|
|
Part 9:
|
Picato Gel Ingenol mebutate in varying strengths is used in the treatment of Actinic keratoses.
The 3 day treatment for face lesions uses 0.015% strength while the 2 day treatment on the limbs or trunk uses 0.05% strength.Suggested treatment areas covered by the supplied doses of gel are 25 cm2 which is not great! On the face avoid around the eyes, lips and nose.The variability of individual patient reactions with Picato is my biggest problem. Some people get blistering after only the first application.Very rare anaphylactic reactions have occurred. If it gets in the eye corneal burns have occurred. The following is from the company website on side effects in the trials. "The most common adverse reactions observed in clinical trials on the face and scalp (=2%) are local skin reactions (94%), application site pain (15%), application site pruritus (8%), application site infection (3%), periorbital edema (3%), and headache (2%). The most common adverse reactions observed in clinical trials on the trunk and extremities (=2%) are local skin reactions (92%), application site pruritus (8%), application site irritation (4%), nasopharyngitis (2%), and application site pain (2%)."
None the less the product has a place especially on the scalp and lower legs and backs of hands where a field treatment for actinic keratoses is required.
|
|
|
Part 10:
|
Latest therapies for severe localised and disseminated nonmelanoma and melanoma skin cancers. See the BRAF inhibitors above for melanoma.
Gefitinib - This is a tyrosine kinase inhibitor that has been successfully used in locally advanced SCC.
Cetuximab - This is a monoclonal antibody directed against epidermal growth factor and used as an adjunct with radiotherapy or chemotherapy in the treatment of severe SCC of the head and neck.
Google these two drugs if you require more information. They are very expensive!
Latest drugs for BCCs.
ODOMOZO ( sonidegib) is a hedgehog pathway inhibitor for adult patients with locally advanced BCC not amenable to curative surgery or radiation therapy or Metastatic BCC. Can cause fetal death Pregnancy Category X.
|
|
|
|

















No comments:
Post a Comment