AN Australian study has provided evidence that sunscreen can help prevent melanoma, perhaps answering a key question at the core of sun safety.
Despite evidence that sunscreen can protect against less lethal forms of skin cancer, its effect on the incidence of rarer but often deadly melanoma has remained unclear.
However a study which tracked a group of just over 1600 residents in Nambour, Queensland, showed how wearing sunscreen every day cut their incidence of melanoma in half.
The study by Queensland Institute of Medical Research Professor of Epidemiology Adele Green randomly allocated adults to either a control group - who wore as much or as little sunscreen as they liked - or a group given an unlimited supply of sunscreen.
Those provided with free sunscreen were asked to apply it every morning to their head, neck, arms and hands in a trial that ran for five years to 1996.
Monitoring over the next 10 years identified 22 cases of melanoma in the control group, and 11 cases among those who wore sunscreen every day.
Professor Green said while the result appeared to be conclusive it was too early to declare the sunscreen-melanoma debate as over.
“I wouldn't say that on the strength of one study but this has to be reassuring at this stage,” she said.
“... to medical professionals, public health authorities and the general public, that the regular application of sunscreen is likely to be beneficial with regard to melanoma protection.”
Professor Green said it has proved very hard to disentangle whether sunscreen protects against melanoma.
Complicating the research has been the fact that very fair-skinned people, who have the most cases of melanoma, are also most likely to heed the warning and so routinely slop on their sunscreen.
“People who are at naturally higher risk of melanoma are also naturally the people who use sunscreen,” said Professor Green.
“There can even be this confusing effect where ... there's more melanoma among people who use sunscreen.”
So while sunscreen has long been recommended as a “precaution” against all skin cancers, the science on its effect on melanoma alone has remained “highly controversial”.
There are three major types of skin cancer, with melanoma the least common but most often lethal, as the cancer can spread from its initial site on the skin to generate tumours elsewhere in the body.
The other types - basal cell carcinoma or squamous cell carcinoma - are more regularly seen but are less likely to spread and so are not usually life-threatening if detected early.
There are more than 10,000 cases of melanoma diagnosed every year in Australia, which shares the world's highest incidence of melanoma along with New Zealand.
More than 430,000 Australians are treated every year for non-melanoma skin cancer.
Professor Green's paper is published in the Journal of Clinical Oncology.
AAP
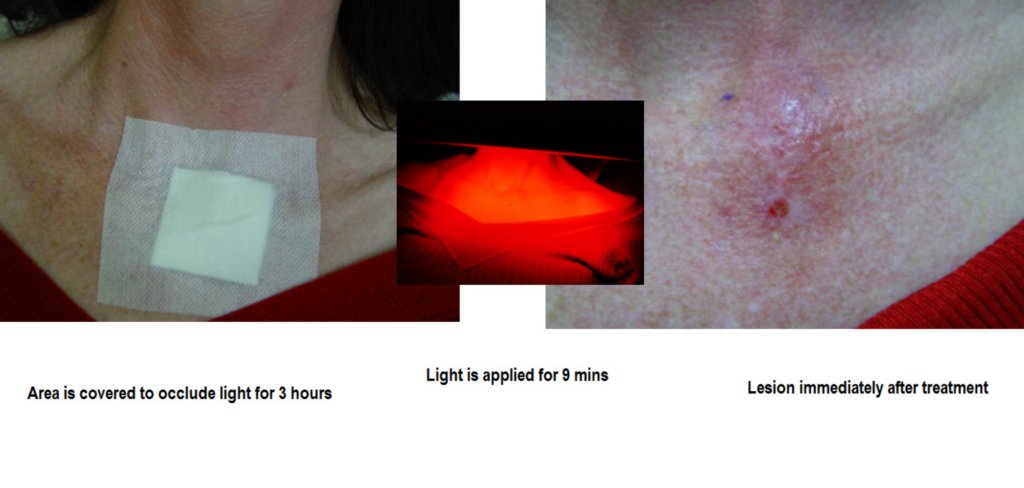
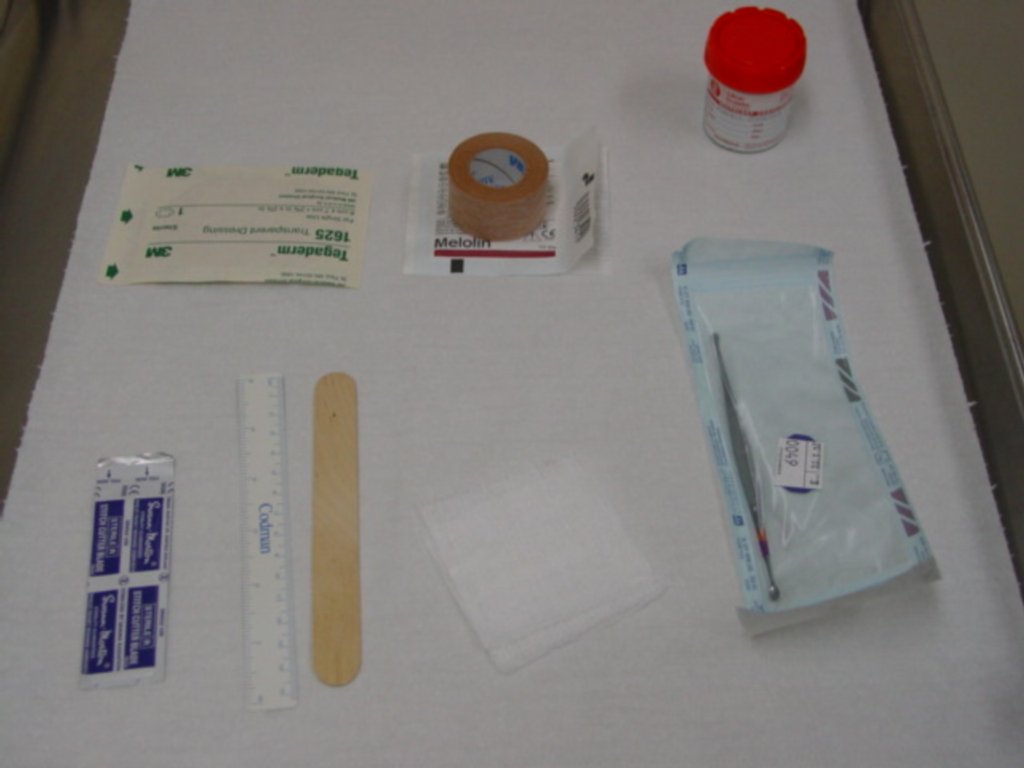
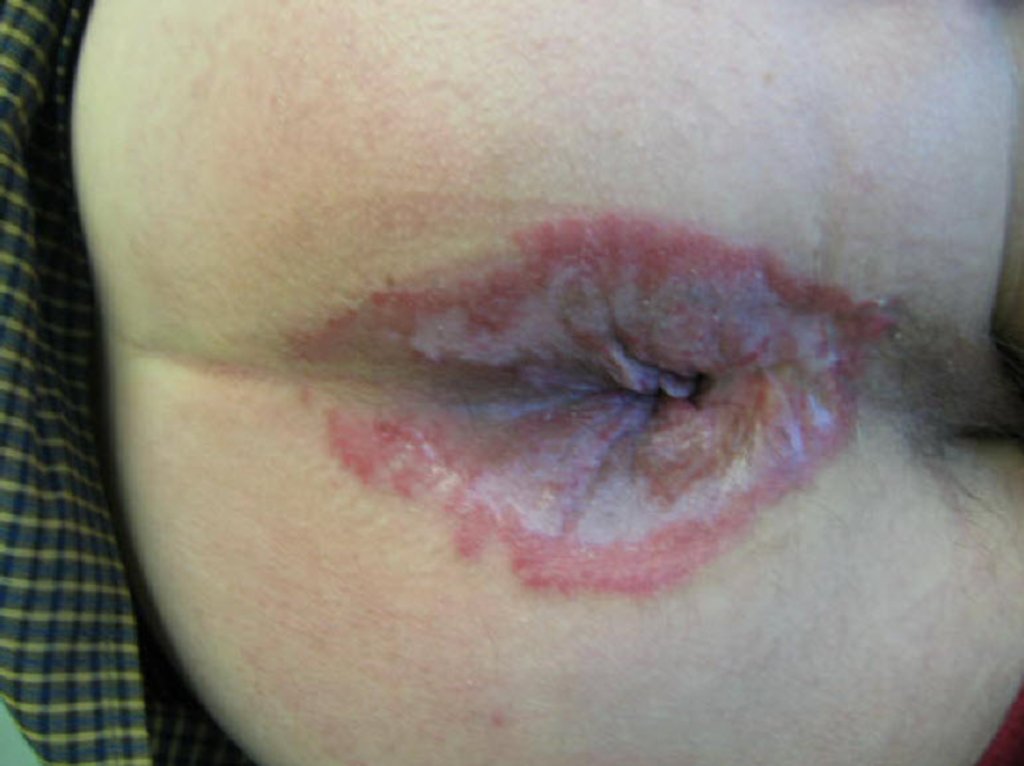
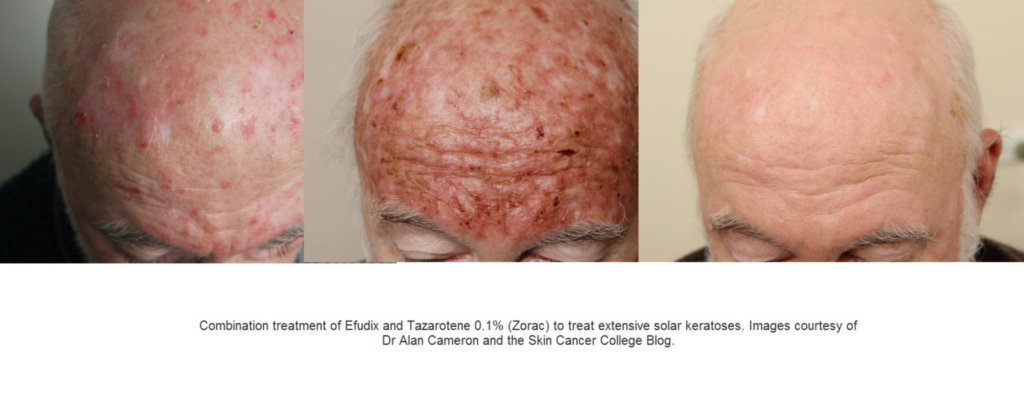
Revise what you have learned so far by reading through
This Dermnet Summary of photo damage topical therapies.














No comments:
Post a Comment